JOINT STATEMENT: UNITED TO END AIDS
Dr Saia Ma’u Piukala, WHO Regional Director for the Western Pacific Region
Eamonn Murphy, UNAIDS Regional Director for Asia-Pacific and Eastern Europe and Central Asia
Manila, 19 June 2026 – “UNITED TO END AIDS”, a new UNAIDS report released ahead of the 2026 UN General Assembly High-Level Meeting on HIV/AIDS, sends a clear warning: progress against AIDS is real but fragile.
The devastating funding disruptions of 2025 have exposed how vulnerable HIV responses remain.
Countries have moved quickly to protect treatment when external support was suspended, reduced or delayed.
However, specific programmes that have been under-prioritised in national budgets, including HIV prevention, testing, community-led services and efforts to remove barriers to care, have been hit hard. Without decisive action, these gaps risk fuelling new infections and AIDS-related deaths. Indeed, we are already seeing worrying signs.
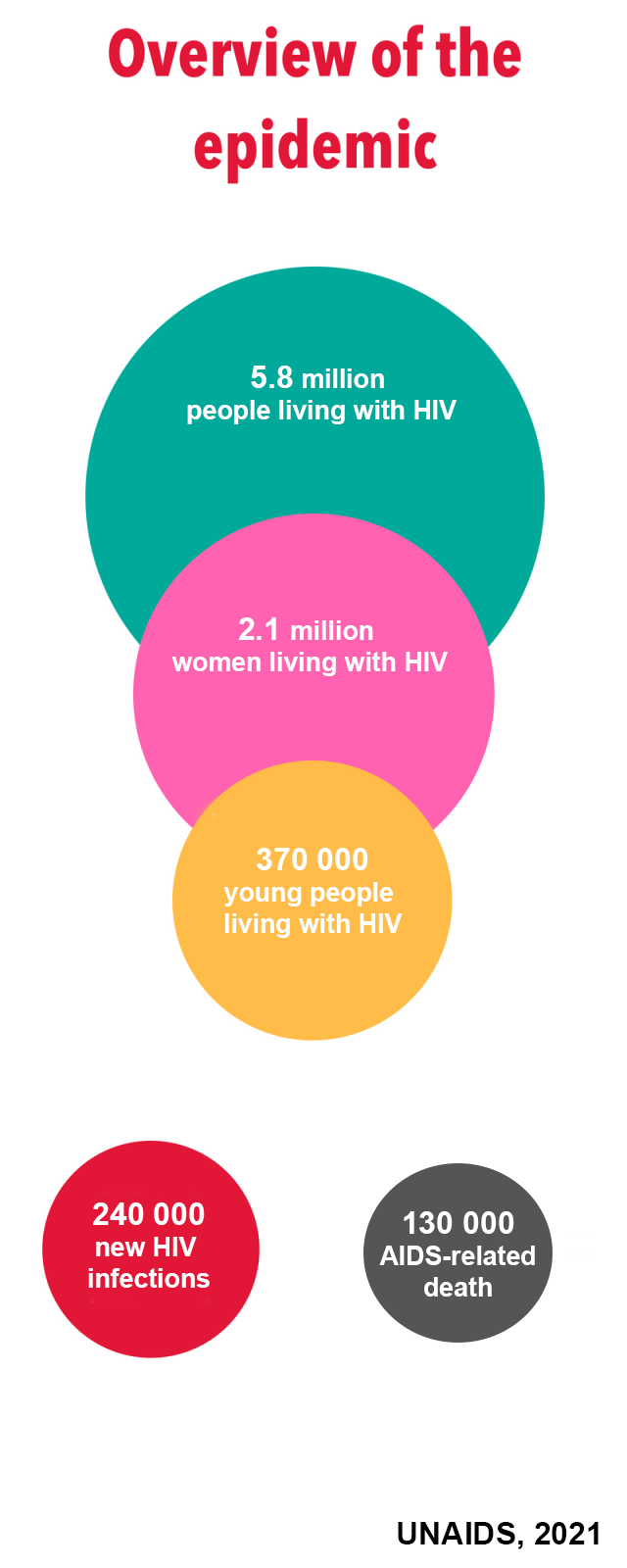
Asia and the Pacific, with 60% of the world’s population, remains home to the world’s second-largest HIV epidemic. Currently, around 7 million people are living with HIV. Each year, an estimated 280,000 people acquire HIV and 120,000 die from AIDS-related illnesses.
Several countries, including Fiji, the Philippines and Papua New Guinea, are grappling with some of the world’s fastest-rising HIV epidemics.
The High-Level Meeting and new Political Declaration must respond to this reality and truly drive the political choices needed to sustain and transform the HIV response.
The Global AIDS Strategy 2026–2031 provides a clear path: country-led sustainability, people-focused services, and community-led response.
Country-led sustainability
The financing landscape has changed drastically. Global development assistance has fallen sharply, and international support for HIV continues to decline.
Our new reality requires a shift away from donor dependence towards country ownership and domestic financing, backed by continued global solidarity.
It is encouraging that across Asia and the Pacific, governments are taking greater responsibility, particularly for treatment.
China, India, Malaysia, Singapore and Thailand finance more than 90% of their HIV responses from domestic resources. Since 2025, 12 more countries have reported plans to increase domestic HIV funding, including Fiji, which has allocated an additional US$4.5 million to its urgent ongoing national HIV response. Papua New Guinea has allocated an emergency fund of US$13.5 million for HIV, tuberculosis and malaria.
But prevention and community-led services remain heavily dependent on international funding. Around 76% of HIV prevention spending in the region still comes from external sources, leaving outreach and community-led services for key populations exposed as international support declines.
Long-term sustainability requires more than replacing external funds. It means integrating HIV into universal health coverage and primary health care, strengthening national systems and data, addressing societal barriers to services, and accelerating access to innovation.
Targeted donor support remains critical in this transition, with UNAIDS, WHO and partners helping countries protect essential services and build sustainable, country-owned HIV responses.
Sustainability will only matter if services reach people
Lifesaving antiretroviral treatment is reaching 5 million people in Asia and the Pacific, but nearly one third of people living with HIV are still not receiving it. The regional treatment coverage remains at 71%. Late diagnosis continues to drive avoidable illness and deaths.
Prevention is also far behind: coverage of oral pre-exposure prophylaxis, or PrEP, a genuine game changer in preventing infection, is only around 2.5% of what is needed.
The new UNAIDS report calls for integrated, differentiated and people-focused services.
Across the Asia-Pacific region, the priority is to ensure that prevention, testing, treatment, and care reach those facing the greatest barriers, including people living with HIV, key populations, young people, and migrants.
This means applying evidence, removing service barriers and combining biomedical tools with stigma reduction and rights-based delivery.
We have clear examples of how this approach can work. Cambodia’s achievement of the 95–95–95 HIV treatment targets (95% of people living with HIV know their status, 95% of those diagnosed are receiving antiretroviral treatment and 95% of people on treatment have achieved viral suppression), a first for Asia and the Pacific, sends a clear message to the region and the world: progress is possible when services are designed around people.
Strong political commitment, national leadership, long-term partnership and community trust have expanded access to testing and treatment, multi-month dispensing, stronger links with the wider health system, and innovations such as PrEP and HIV self-testing.
At the seventy-sixth WHO Regional Committee for the Western Pacific last year, a joint WHO–UNAIDS session on HIV and substance use engaged 38 countries and areas around this same priority: making services respond to people’s realities.
Innovations accelerate progress, but only if access is equitable.
Long-acting prevention tools, including lenacapavir as a twice-yearly injectable, could transform prevention for people who face stigma, barriers to daily pills, and regular clinic visits.
Asia-Pacific has major manufacturing potential, with four of the six currently licensed generic manufacturers for lenacapavir based in India and Pakistan, which could support faster product introduction.
But scale-up will require more than new products.
We need to combine technical and normative guidance on health-system readiness with advocacy on equity, affordability, rights, community engagement and accountability in the HIV response.
With this support, countries can turn innovation into people-focused services that reach those who need them most and, in turn, enhance community-led responses.
Community-led governance is crucial
In Asia and the Pacific, communities are essential: they build trust, reach people missed by formal systems, and make prevention and treatment services work in practice.
In Thailand, average PrEP retention is 268 days through key population-led providers, compared with 148 days in public health facilities – clear evidence of the value of peer-led services.
As the new UNAIDS report underlines, community leadership is central to a sustainable HIV response, but funding cuts, punitive laws and shrinking civic space are putting it at risk.
Key populations – including men who have sex with men, sex workers and injecting drug users – remain criminalized in 39 countries across the region, while stigma and discrimination trends continue to push people away from services.
Legal and policy reform must urgently remove these barriers so people can seek care without fear or discrimination.
In this regard, young people are key.
WHO and UNAIDS have partnered with the civil society organisation Youth LEAD to bring together young key populations, governments and partners from 11 countries to co-design HIV and STI prevention roadmaps grounded in community leadership, youth engagement and rights-based services.
As foreign assistance for HIV declines, community-led organisations need funding, protection and a formal role in the HIV response.
Social contracting can help by enabling governments to fund civil society organisations to deliver services and connect community systems with public health systems. Yet this modality remains underused. Among 39 countries in the region with available data, only 35% report laws, regulations or policies that allow domestic funding for community-led service delivery.
Community leadership is not an add-on. It is central to the AIDS response.
UNAIDS brings the political mandate, community partnerships and accountability role needed to help countries protect civic space, advance human rights and make community-led responses a core part of national HIV systems.
The choice before us
The new UNAIDS report explicitly shows what is at stake. The High-Level Meeting and Political Declaration offer the opportunity to act.
Countries in Asia and the Pacific should seize this moment to sustain financing, close gaps, remove barriers, and put communities at the centre.
The next phase of the AIDS response must be country-led, people-focused and community-driven.
The choice is clear: Squander the significant gains made in tackling one of the biggest public health challenges of all time, or safeguard the progress made and go the last mile in ending AIDS for once and for all.
###
For media enquiries, please contact:
Snizhana Kolomiiets, UNAIDS Asia-Pacific and Eastern Europe and Central Asia, at kolomiietss@unaids.org or by telephone at +4915111009830.
Roy Wadia, WHO Regional Office for the Western Pacific, at rwadia@who.int or by telephone at +639189157260.